
Understanding Mucosal Integrity: A Clinical Guide to MiVu™
Understanding Mucosal Integrity: A Clinical Guide to MiVu™
Insights from a virtual physician discussion led by Michael Vaezi, PhD, MD, MS, on how mucosal integrity testing provides real-time, physiologic data to support diagnosis and treatment decisions in GERD, EoE, and Non-GERD.

Expanding the Clinical Utility of MiVu: Monitoring Therapy and Surgical Outcomes
In addition to its diagnostic value, recent clinical studies are reinforcing the value of MiVu to monitor treatment response and assess physiologic outcomes over time.
For patients on proton pump inhibitors (PPIs), mucosal integrity testing provides an objective way to evaluate whether acid suppression is driving mucosal healing. Rather than relying solely on symptom improvement, which can be variable and subjective, clinicians can directly assess changes in the epithelial barrier. This allows for more informed decisions around therapy optimization, particularly in patients with persistent symptoms or uncertain response.

MiVu is also being used following anti-reflux interventions, such as Nissen fundoplication, as an objective physiologic marker of surgical success, supported by a clinical study published in the Journal of Gastrointestinal Surgery. By measuring mucosal integrity after intervention, clinicians can determine whether reflux-related epithelial damage has been resolved, complementing symptom reporting and traditional follow-up methods. This provides a more complete picture of treatment effectiveness and helps guide post-surgery management.
Barrett’s Esophagus
In patients with Barrett’s esophagus, for example, measurements should be obtained from areas of normal-appearing squamous epithelium proximal to the Barrett’s segment, as the tissue itself will inherently demonstrate low impedance. Assessing these proximal areas can help clinicians evaluate whether acid suppression therapy is adequately protecting the remaining esophagus.
Why Develop MiVu™ Mucosal Integrity Testing System for Gastroenterology?
One of the more frustrating realities for gastroenterologists is that the mucosa can appear normal during endoscopy despite underlying pathology. This diagnostic gap helped drive the development of MiVu, which provides a unique, point-of-care assessment of mucosal integrity using mucosal impedance to evaluate the epithelial barrier. Low impedance reflects altered epithelium, whether due to acid, bile, inflammation, or mechanical factors.
MiVu also addresses the limitations of pH testing, which measures acid exposure at a single location in the esophagus over a 24-96-hour period. MiVu assesses mucosal integrity along a 10 cm segment of the esophagus during an endoscopy, providing an immediate assessment of epithelial health. For clinicians and patients, this offers several practical advantages:
- Reduced behavioral bias: During pH testing, patients often alter their diet, activity, or medication use, which can influence test results.
- Less patient burden: MiVu avoids the discomfort associated with nasal catheter placement and the inconvenience of monitoring their activities.
The Clinical Problem: When the Esophagus Looks “Normal”
Gastroenterologists are trained to visually assess the structural integrity of the esophagus during endoscopy to identify erosive esophagitis, strictures, Barrett’s esophagus, and other esophageal conditions.
- In early GERD, damage may be limited to the distal esophagus and hard to visually identify during an endoscopy procedure.
- In eosinophilic esophagitis (EoE), alterations can be patchy, subtle, or diffusely present and easily missed if biopsies don’t sample the right area.
- In non-erosive reflux disease (NERD), patients experience chronic/classic reflux symptoms, yet the esophagus shows no inflammation during a traditional endoscopy.
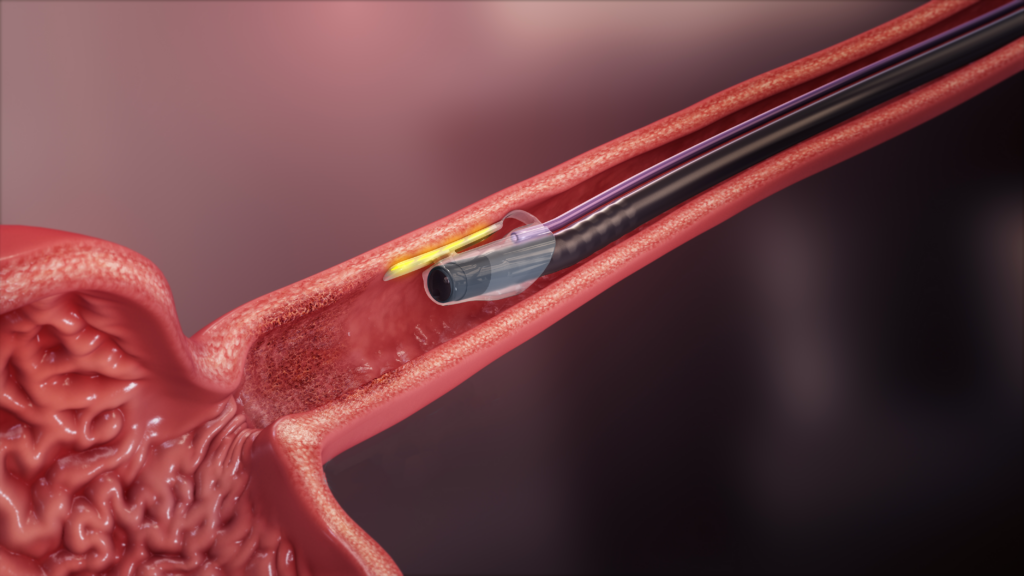
How Does MiVu Measure Mucosal Integrity?
MiVu is easy to use with intuitive software that helps physicians successfully capture readings along the esophagus. Clinicians securely attach the disposable Endo Cap to the distal end of the endoscope and properly position the sensors against the mucosal wall to capture high-quality measurements. Immediately, the system generates distinct color-coded patterns that help gastroenterologists differentiate GERD, EoE, or Non-GERD, providing objective data to support clinical diagnosis and treatment plans immediately following the procedure.
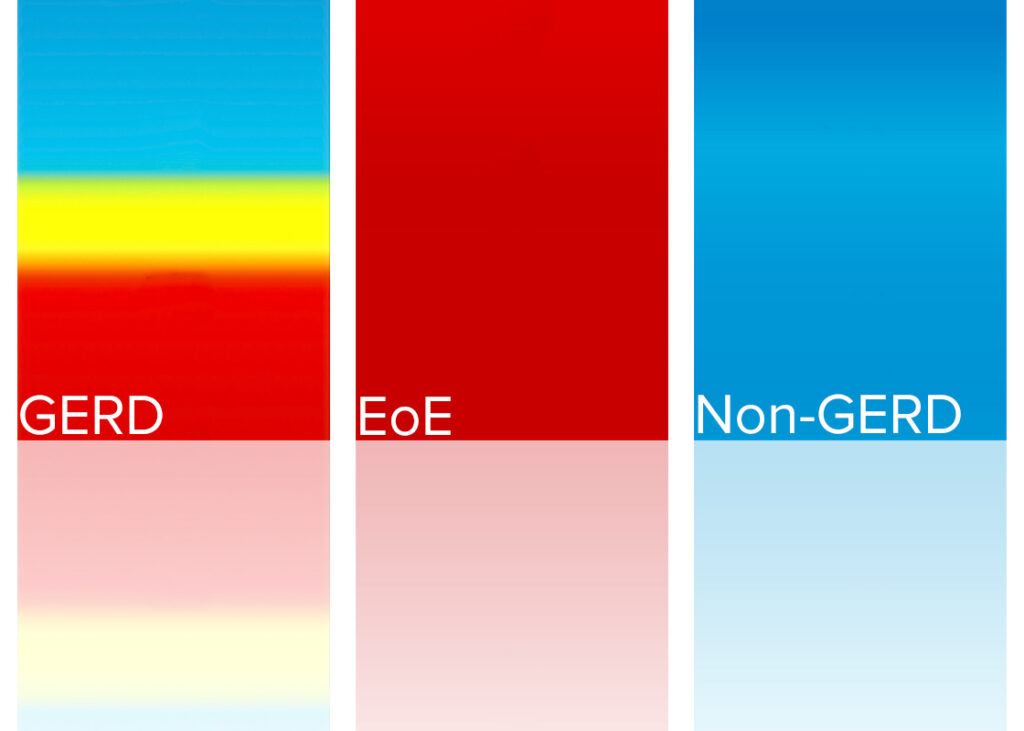
- GERD typically shows lower impedance (epithelial alteration) in the distal esophagus.
- EoE often shows low impedance (epithelial alteration) throughout the esophagus.
- Non-GERD maintains higher impedance values throughout the esophagus.
Interpreting MiVu: Pattern Recognition and Clinical Reasoning
Initially, the software assigns equal probability — 33.3% each — to EoE, GERD, and Non-GERD. As measurements are acquired, these probabilities are adjusted based on the resulting pattern of impedance values.
The software assigns probability. Clinicians make the diagnosis.
The real value for physicians lies in assessing pattern recognition; understanding it can range from altered mucosa limited to the distal esophagus to pan-esophageal alteration. The reliable, easy-to-distinguish results from MiVu, combined with patient history, demographics, and other clinical findings, empower clinicians to make a confident, point-of-care diagnosis and create an individualized treatment plan.
Best Practice Tips to Maximize MiVu’s High Accuracy
Like any diagnostic tool, interpretation requires context. False positives may occur with a foamy esophagus. Clinicians should clear and suction residual foam and saliva before performing the MiVu test to obtain high-quality measurements.
False positives can also occur when MiVu is performed after an esophageal biopsy, as blood appears as a liquid for the impedance measurement. Clinicians should perform MiVu before taking biopsies of the esophagus.
Air trapped between the sensors and the esophageal wall can artificially increase impedance, leading to false negatives.
Physicians should consider that false negatives may occur in patients on PPI therapy, as the impedance values appear normal, indicating the PPI is working, even though the patient carries a definitive diagnosis of GERD.
Practical Insights for Physicians Using MiVu
The following guidance reflects insights from Michael Vaezi, PhD, MD, MS, Professor of Medicine at Vanderbilt University and a leading contributor to the clinical development and evaluation of mucosal integrity and MiVu.
- Focus on patterns. When interpreting real-time results, focus on the overall distribution or pattern of impedance values along the esophagus rather than individual probability scores.
- Integrate findings with clinical context. MiVu should complement, not replace clinical judgement. Incorporate the patient’s symptoms and overall health history to build a comprehensive understanding of esophageal disease.
- Minimal learning curve. The technology is intuitive and integrates easily into existing EGD workflows.
Growing Clinical Adoption of MiVu in Gastroenterology
The recent implementation of the MiVu™ Mucosal Integrity Testing System at Schoolcraft Memorial Hospital reflects how mucosal integrity testing supports esophageal diagnosis and management through objective, point-of-care data.
As Dr. Medhat Fanous noted, “Mucosal integrity testing lets us see, in real-time, whether the esophageal lining has been damaged by acid. That means fewer inconclusive results, fewer follow-up tests, and a faster path to the right treatment”.
Recent Posts
Contact Us
+1 800 558 6408 or +1 414 265 7620
General Inquiries: sales@diversatekhc.com